 0
0 Spinal flexion – what it means for bad backs and osteoporosis
Fri,Nov 11, 2016 at 02:48PM by Carla Mullins
Let’s talk about flexion of the spine
Flexion of the spine appears to be one of those discussion points at ever so many training courses. It is not the topic of the course mind you, but the sort of question or idea that people raise and the conversation seems to be about ideas that need to be thought through or discussed just that little more. The comments go something like this:
“People are in flexion all day because they sit; surely we shouldn’t be having them do more in their exercise class”
“Flexion induces the stress and fear response”
“Flexion is not good because of osteoporosis”
“Pilates is far too flexion-based”
All of these are questions I have had over the years and I admit that it has taken me a long time to get there and think and consider the arguments through in detail. I am finally at peace with flexion and its role in movement, particularly given that there is so much flexion in pilates, gyrotonic and normally in everyday life. This article is about flexion, what it is, its role, its benefits and dispelling some of the myths and clarifying some understanding.
What are we talking about when we use the term flexion?
I like to start with the understanding that at birth our body has a primary curve, which is best described in a movement perspective as “C curve “ (pilates) “Curl”(Gyrotonic) and “Curling” (Aston Technique). This primary curve is a flexion of the spine with flexion assisted by gravity in the limbs. As we progress to upright beings, we start to develop secondary curves in our spine partially as a response to the pull of gravity, and this is what happens when we start to achieve extension. As a consequence, we should have a certain amount of resting flexion in our thoracic and sacral regions of the spine and resting extension in the cervical and lumbar regions. This is what we would generally understand to be good alignment or posture when upright. Our limbs (humeri and femurs) in upright postural resting position are in a slightly internally rotated, or flexed position when we are responding to gravity.
Why is flexion good?
When we move about our daily life we need to be able to flex the spine. Here are simple tasks that I am suggesting are not possible without flexion of the spine:
// Putting on your underpants or bra
// Putting on your shoes
// Washing your face
// Hugging a child
All of these are just simple daily tasks that require range of motion in the spine. When we deny the body a range of motion, then we need to consider how we are going to limit further movement in our spine, contribute to the loss of muscle mass, strength and postural control.
What we should be considering when we discuss about spinal movements?
Rather than just thinking about flexion or extension, let us remember all the spinal movements and the differences of those possibilities at different segmental levels of the spine.
Remember that the spine has the capacity to:
// Flex
// Flex and rotate
// Flex and side bend
// Extend
// Extend and side bend
// Extend and rotate
// Side bend and rotate
Ultimately, in a good movement class we are looking to achieve or work towards all of these movement possibilities. Yes, there will be situations when a person cannot or should not move a segment of the spine because of injury or pathology, but those limitations should be recognised as one area of the spine, and that mobility should still be maintained elsewhere in the spine. Furthermore, we should eventually be working towards safe movement potential in the spine.
Often the problem we see in a movement class is that the person has failed to achieve potential movement and as a result has compensatory patterns. A good movement class addresses these patterns and educates the body and person as to what is healthy stability and movement. In other words, a good movement teacher adjusts their work to the client before them rather than following a formula.
We have to be careful of loaded flexion because of the risks on structures of the body such as joints and discs. Hopefully common sense prevails so that we understand exercises like short spine need to be carefully evaluated before they given to people. Furthermore, that short spine and tower and such are not just flexion exercises they are complex exercises requiring strength and stamina. For them to be given to a client, the client must have been able to achieve a whole series of benchmarks in movement and flexibility.
Myth one: sitting means our “spine” is in flexion
When we sit we naturally change our spinal alignment, depending on the angle of the hips. If our femurs are sitting at 90 degrees or more of flexion, then the femoral head is going to be sitting deeper in the socket and therefore forced into a more significant internal rotation which naturally results in a small flexion of the lumbar spine, that flattens the lumbar spine out rather than fully flexing the spine. This can be attributable to the role of the psoas major, which at the L5 and L4 levels, is responsible for pulling the spine into flexion. When the psoas is shortened at the hips it naturally creates the pull on the lumbar spine into that slight flexion position. However, as one part of the body is placed into partial flexion, the rest of the body does not always follow into that pattern, and so there is not a full experience of flexion.
Experiential
Try sitting on your chair with knees at hip height notice what happens to your lumbar spine, and your neck, particularly as you read this article.
My suspicion is that you will find that your:
// L5-L4 has flattened and L2 and L1 has extended a bit more,
// Your lower thoracic spine has extended,
// Your upper thoracic spine has increased its flexion,
// Your head has moved forward so that at the points closest to the skull the cervical vertebra are extended in the upper quadrants only.
I like the image below to show what does happen.
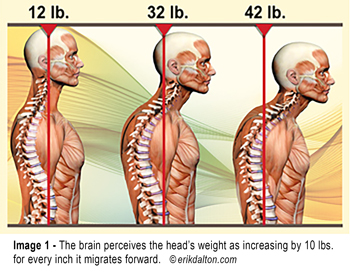
Having been through this experience we start to realise that the body is not necessarily in more flexion from sitting down all day, but rather a whole series of changes in the overall posture occur because a small part of the lumbar spine has started into flexion and not necessarily completed its pattern into full flexion.
Accordingly, when we talk about flexion, we are not talking about one particular segment of the spine but the relationships of the various spinal curves as parts balance in extension and other parts in flexion. An excessive movement in one part of the spine plays out elsewhere, resulting in changes in the overall balance. A simple avoidance of a movement because we consider one part of the spine as being already too flexed or too extended is a failure to appreciate the interconnectedness of the spine and body and its capacity for movement.
Does a stand-up desk help?
Standing up will vary our postural responses, but if that is the only solution to staying at a desk all day it is probably not going to be a long-term solution. Remember, when we stand we still have our postural habits and if we are still standing looking at a computer screen, we again start to see all sorts of poor postural compensations particularly with excessive extension of the neck, gripping in the hips or hinging in the back particularly when a person starts to fatigue.
Myth two: flexion induces the stress and fear response
This is one I have heard a lot, particularly in yoga circles, but to get to the bottom of the basis of this comment is difficult. I personally don’t really understand the assertion.
My understanding is that the “startle response,” which results in us moving back into extension, and the calming of that response is to curl forward into flexion. Think about what happens when a healthy person hears a loud noise, it is the back extensors that tighten and we then relax by curling forward. It is not flexion that is the response to fear, but rather, the bodies solution to stresses on it, some could conclude that there is a biomechanical response to protect itself.
Avoiding flexion because of a psychological response rather than a physical need for the body to complete a pattern of movement is not necessarily a good solution for us all. If anyone can give me a greater insight into why this belief exists and where it comes from it would be much appreciated.
Myth three: flexion is bad because of 0steoporosis
Osteopenia is not osteoporosis
When I am told by practitioners that flexion is bad because of osteoporosis, my first question is; do you know if your client has osteoporosis and, if so, at what degree of bone density? (That is a bone density T score of -1.8 or less) If the answer is that they don’t have osteoporosis but rather osteopenia, I try to have them understand the inter-relationship between sarcopenia and osteopenia.
Sarcopenia
Sarcopenia is the loss of muscle mass and strength associated with ageing, and it is linked with low BMD and an increased risk of fracture1,2,3,4,5,6. The degenerative processes leading to osteoporosis and sarcopenia show many common pathogenic pathways. Genetic, endocrine and mechanical factors, as well as inflammatory and nutritional states have been found to concurrently affect both muscle tissues and bone metabolism4. The strongest mechanical forces applied to bones are those created by muscle contractions that impact upon bone density, strength, and microarchitecture. Not surprising, therefore, that a decrease in muscle strength leads to lower bone strength. Conversely, clinical data has indicated that increased muscle mass is related to increased bone mass and reduced fracture risk.
Accordingly, strengthening muscles in all ranges of movement are necessary for maintaining good muscular and bone health. Avoiding a movement because of fears about fractures etc that are not relevant is not allowing your client to receive optimum health and balance.
Myth four : pilates is too flexion-based
I often hear this sort of comment from people who get a “sore neck” from too much head lifting work in pilates. The problem in this case can be linked more to the teacher’s failure to cue or correctly modify work for clients unable to appropriately curl at the chest rather than extend at the neck. In those situations I suggest that the person support the head with a towel so that the neck remains in a good position rather than extending as the person prepares for chest lift, and learns to control and progress to unsupported chest lift work.
Pilates has a whole series of movement patterns and shapes of the spine that are exhibited in its repertoire. To fully appreciate pilates we need to ensure that the movement patterns are representative of all the movements of the spine. A balance movement class would have incorporated the flexion abdominal series but also a lot of other work from sides, four point kneeling to extension.
Finally, let us remember that Joseph Pilates was an asthmatic and as such would experience problems in the exhale. Accordingly, it is of little surprise that so much of his work revolves around improving the exhale and descent of the diaphragm in the abdominal series. However, what works for him may not always be relevant to others and therefore teachers do not need to change their focus on abdominal flexion based exercises to broader spinal flexion and broader spinal patterning in order to meet the needs of their clients.
What makes good spinal flexion in a movement class
When we are wanting to achieve flexion of the spine we are wanting to consider and ensure that the patterns described below are all possible. Furthermore, we need to remember the consequences of the joint, muscle and disc changes.
// Flexion at the sacral level requires the illia to open out and around so that sacrum can float backwards. Rectus abdominus will contract and create the pull on the pubic rami so that the illia are pulled forward as the sacrum floats backwards.
// Therefore requiring the femoral heads to spiral into an internal rotation allowing psoas major to contract at the L5/L4 levels whilst Piriformis lengthens. At the T12 level, psoas is eccentrically lengthened so that the Diaphragm can lower and pull the ribs anteriorly.
// When flexing the spine, the intervertebral discs will be compressed anteriorly and open posteriorly.
// As the ribs are pulled anteriorly, the vertebral bodies of the thoracic spine are pulled further into flexion. The humeral head and the skull are then alo required to sit slightly flexed in order to allow the flexion of the upper thoracic and upper cervical vertebrae.
// The collar bone spirals forward and down and the scapula will therefore elevate and protract.
// The hyoid bone shall change position, at the C3 level , and therefore so will the tongue. The tongue shall float down and curl into the back of the lower teeth.
To learn more about spinal movements, try our online Anatomy Dimensions Spine and Torso course .
References
-
- Interaction between Muscle and Bone- Hiroshi Kaji J Bone Metab. 2014 Feb; 21(1): 29–40. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970293/
- Osteoporosis and sarcopenia: the connections. Tarantino U1, Baldi J, Celi M, Rao C, Liuni FM, Iundusi R, Gasbarra E. Aging Clin Exp Res. 2013 Oct;25 Suppl 1:S93-5. doi: 10.1007/s40520-013-0097-7. Epub 2013 Sep 18. http://www.ncbi.nlm.nih.gov/pubmed/24046056
- Sarcopenia and fragility fractures. Eur J Phys Rehabil Med. 2013 Feb;49(1):111-7 Cederholm T1, Cruz-Jentoft AJ, Maggi http://www.ncbi.nlm.nih.gov/pubmed/23575205
- Interactions between muscle tissues and bone metabolism. Kawao N1, Kaji H. J Cell Biochem. 2015 May;116(5):687-doi: 10.1002/jcb.25040 http://www.ncbi.nlm.nih.gov/pubmed/25521430
- Di Monaco M, Vallero F, Di Monaco R, Tappero R. Prevalence of sarcopenia and its association with osteoporosis in 313 older women following a hip fracture. Arch Gerontol Geriatr 2011; 52: 71-74.
- Verschueren S, Gielen E, O’Neill TW, et al. Sarcopenia and its relationship with bone mineral density in middle-aged and elderly European men. Osteoporosis Int 2012; Jul 10 [Epub ahead of print http://www.who.int/chp/topics/Osteoporosis.pdf (written 2004)
- Clinical practice guideline for the prevention and treatment of osteoporosis in postmenopausal women and older men. http://www.racgp.org.au/your-practice/guidelines/musculoskeletal/osteoporosis/Melbourne: RACGP, 2010